Dimensional and categorical approaches to brain-behaviour relationships in reading disorder (dyslexia)
")
Executive summary
- Reading disability (dyslexia) is best described as an impairment in learning the written-form of a language.
- Dyslexia is typically diagnosed using behavioural measures of reading achievement, but the causes are most likely to be found within the underlying biological and cognitive mechanisms.
- Dimensional approaches to understanding individual strengths and weaknesses as continuous variables and across multiple levels level of observation – from genes, brains and behaviour – offer powerful alternatives to existing perspectives of dyslexia as a disorder specific to reading.
Specific reading disability: Category or continuum?
Unlike other neurodevelopmental disorders, such as attention-deficit hyperactivity disorder or autism, dyslexia (specific reading disorder) is not typically considered a medical issue, and therefore diagnosis is made by a wider range of professionals, including educational, occupational or clinical psychologists, or specialist teachers with a background of working with persons with special educational needs. Because dyslexia sits between education and mental health assessment, practitioners may apply different rationale, evidence and assessment measures to derive a ‘diagnosis’. If the rationale for diagnosis is to identify individual children with low achievement and who would benefit from specialised support for their educational development, then the main assessment issue for the professionals involved is how effectively can they identify such children. This process is much less useful, however for understanding the underlying mechanisms of disorder and for developing taxonomic structures, toward identifying patterns of deficits across individuals that are sufficiently homogeneous to be considered as independent diagnostic entities.
That some children are poorer readers than others is indisputable and that some are poorer than might be expected given their profile of other cognitive abilities is also certain. What remains unclear, however, is whether poor readers are best described as statistical outliers or whether they form a distinct subgroup from typical readers1,2. This debate, between dimensional and categorical approaches to children with reading difficulties/dyslexia, has been revived by the decision to replace the term ‘dyslexia’ in Diagnostic and Statistical Manual (DSM-5)3 with ‘specific learning disorder (reading)’, and subsequently by resurgent claims that dyslexia is an unscientific construct that provides little help, either in explaining the mechanisms of reading difficulty or to predicting educational outcomes in those affected4,5. This debate is important because the true nature of reading difficulties has powerful implications for how we frame and deliver the diagnosis, intervention and service provision that is needed for those affected. In part, this issue arises from the dual roles of assessment practice and in the search for taxonomic systems that demonstrate utility in discriminating between groups. Current assessment practice is very good at identifying distinguishing features of disability at the individual level, but this process is conceptually different from that of taxonomic classification, based on the aim of identifying and grouping cases from the characteristics that distinguish them from other individuals or other disorders.
Developmental dyslexia has a long and storied history with respect to its operational definitions, running from initial descriptions of ‘congenital word-blindness’ in the late 19th century6, to current diagnostic criteria as a specific learning disorder in the current revision of the DSM3. Current diagnostic criteria for dyslexia is as an alternative term for a specific reading disorder, describing symptoms manifest in text-based language learning including: a persistent pattern of difficulties in learning to read; inaccurate or slow and effortful reading at a level below that expected for (typically) a child’s chronological age, and, difficulties in literacy achievement that is not accounted for by obvious disabilities in other endogenous (e.g. intellectual disabilities) or exogenous (e.g. lack of educational access) factors.
Assessment practice for identifying dyslexia is conventionally based on applying individually administered, standardised tests of achievement in reading, and of literacy-component skills, alongside measures of general ability in both verbal and non-verbal domains. Standardised tests enable the assessment of an individual child’s level of achievement, compared to other children of the same age who have contributed to the standardisation sample. Using these measures, a statistical definition of impairment is derived, and this is most often based on a pre-defined cut-off score at some point below the average in the population distribution of performance on that measure. Unfortunately, when used to identify children with difficulties, this method involves applying somewhat arbitrary statistical cut-offs in the continuous data obtained from the tests to define the impaired and unimpaired categories on a measure. Conventionally, this involves setting a cut-off of 1, 1.5 or 2 standard deviations below the mean of reading ability for the referent age group. Unfortunately, these cut-offs are as much determined by convenience as they are by any principle or an empirical evidence base7, and it is obvious that procedures of this type will inevitably identify groups of children on both sides of the cut-off point, regardless of whether dyslexia exists as a coherent entity or not. As would be consistent with a rather non-specific set of diagnostic criteria, the estimated prevalence of dyslexia in the population varies widely, depending at least in part on the number of children that are captured by these variously defined statistical criteria or disorder8,9.
Alongside standardised testing, assessment of dyslexia also applies exclusionary criteria, based on prior and current case history, to rule out other potential causes that could explain the reading achievement deficit in an alternative way, for example, the presence of low IQ, underlying sensory or neurological impairment, or obvious environmental factors. By this process, dyslexia is based on a process of ruling out other causal factors, other than the presence of low reading achievement (where ‘low’ is more often than not defined arbitrarily). While such a process may be effective in identifying children who are not meeting educational benchmarks for their reading achievement, it fails to specify either core deficit criteria or underlying mechanisms, beyond those of the main behavioural symptom set (i.e., lower than average reading achievement). As a consequence, a current diagnosis of dyslexia is highly sensitive to the nature of the assessment procedures, including which tests are administered and by whom, and how diagnostic thresholds are determined. Multivariate methods, such as identifying children based on discrepancies between their obtained and their predicted reading ability (e.g. that based on a regression of reading achievement on cognitive ability), share the same limitations, but will, of course, identify different individuals.
In summary, the methods conventionally used to identify children with dyslexia or specific reading disorder typically share two features. First, they will identify a group of poor readers, irrespective of whether or not any distinctive difference between groups, exists. Second, the categories themselves are arbitrary and are not necessarily based on valid qualitative differences or discontinuities in patterns of continuous data. The consequence of these approaches is that dyslexia is also inconsistently defined in the scientific literature, as the criteria used are variable and their validity is unknown. It seems likely that many of the inconsistent findings reported in the research literature and the controversies they inspire with respect to diagnostic systems, result at least in part from such failures of definition.
Focusing on symptom dimensions: Genes to brains and behaviour
The standard approach adopted by educational systems and researchers alike is to classify children categorically according to the particular area (e.g. reading or mathematics) in which they are experiencing problems, and thereby applying a diagnostic label (e.g. dyslexia or dyscalculia) if the difficulties are severe enough. This pragmatic approach has considerable benefits for the individuals who meet the diagnostic criteria adopted, but many children with relatively mild (i.e., those that do not meet the diagnostic threshold) problems go undetected, particularly if the statistical cut-offs chosen are very conservative. The needs of other children with complex learning difficulties and co-occurring disorders may also go unaddressed.
In response to these shortcomings in current diagnostic practice, research in learning and learning disorders is beginning to move toward circumventing those diagnostic models based on rigid adherence to pre-existing categories of disorder, to focus more on the use of symptom dimensions10. Dimensions capture better the continuous nature of most measures, such that individual performance can be described in terms of continua and across different levels of analysis (genetic risk, brain structure and function, cognitive performance and observed behaviour). This approach to focus on symptom dimensions both within and across disorders is central to the emerging Research Domain Criteria (RDoC) framework11 and is particularly well-fit for studying the heterogeneity of symptoms demonstrated by children both within and between putative diagnostic categories10. To date, the RDoC framework has been most extensively applied to adult psychiatric conditions12,13, but is now finding traction in the study of childhood disorders with a neurodevelopmental basis, and including disorders of learning such as dyslexia10,14.
A key advance of such revised approaches to classification is they apply more data driven methods to identify groups of individuals with similar underlying symptom patterns but without particular reference to pre-existing disorder categories10. Such approaches can be applied to a range of participant samples, broadly sampled deficit groups or within group comparisons, for the analysis of the potential importance of within category variability in the mechanisms and in the developmental progression of the difficulties over time15. Within this latter perspective, the understanding of how reading skill develops in children and what goes awry in reading disorder, now incorporates a range of convergent methods from genetics, through brain imaging, to fine-grained analyses of cognition, and including how these dimensions change over development and in response to variability in learning environments.
The search for the causes of reading impairments has historically been based on testing the predictions of unitary deficit accounts of dyslexia, those that attribute reading difficulties primarily to a single underlying and core causal mechanism. Of these grand causal theories of dyslexia, the most well-developed explanatory framework posits that reading impairment results from the persistent difficulties some children have in learning and using the phonological principles that govern the relationships between letter units and speech sounds within a given written language. Space precludes a formal review of this and alternative causal accounts in this brief; the reader is therefore referred to the following sources as reference17-20. A good deal of previous research on dyslexia was based on testing the explanatory sufficiency of these specific causal theories and cast in discussions about the necessary and sufficient conditions for reading impairment. Revised models that focus on multiple mechanisms approaches to dyslexia cast the debate in a somewhat different light, partly through the increased appreciation that these existing theories make predictions about causal mechanisms of dyslexia that are not necessarily incompatible with one another, but instead are based on observations across different domains (levels) of analysis, each potentially relevant as a dimension of risk for reading difficulties. For example, the phonological and cerebellar accounts of dyslexia might not be as incompatible as proposed, based upon their frameworks associated with observations across the cognitive and neurobiological domains, respectively.
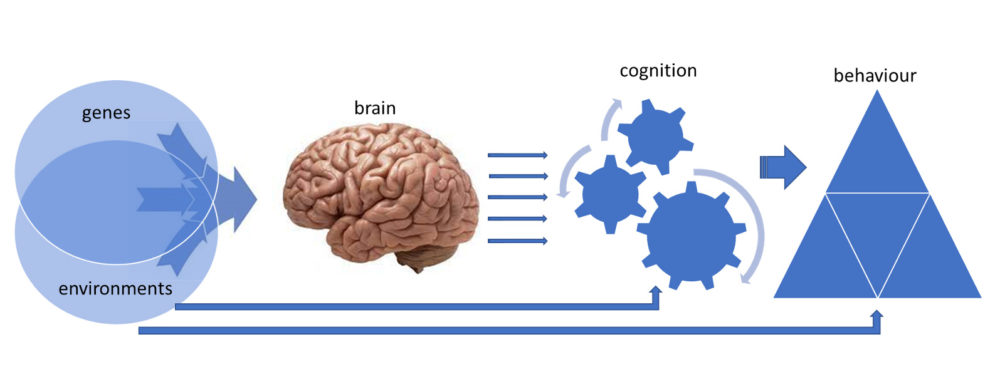
Figure 1. A multilevel framework for conceptualising underlying mechanisms of neurodevelopmental disorders, and of their relationships across different levels of analysis. Key behavioural dimensions, which currently serve as the primary basis of disorder diagnosis and classification are underpinned by a set of cognitive and biological risk factors, with variable expression and impact across individuals.
There is now increasing recognition that there are multiple routes to reading impairments, that are significant enough to warrant a diagnosis of developmental dyslexia21. An example of such an approach is shown in the schematic in Figure 1. Such multilevel explanatory frameworks for understanding neurodevelopmental disorders focus on different levels of explanation with respect to their underlying causes: the biological, the cognitive, and the behavioural16 and are strongly compatible with the data driven, diagnostic agnostic approach, encapsulated by the RDoC framework. These alternative models are moving toward incorporating multivariate, dimensional perspectives that enable disability to be modelled as a continuous variable, based on an estimate of aggregated risk across a set of underlying dimensions, and across different levels (domains) of analysis.
How the brain implements reading and how this goes awry in the biology of developmental dyslexia
Reading in the brain is implemented through the experience of learning to read and imposed on the existing biological structure (the brain). Reading is not innate and needs to be taught, through the learning of the systematic relationships between the visual units and speech sounds that characterise a written language, and which provide a key mechanism for learning new words. In the human evolutionary timescale, the ability to learn and use written language is a relatively new behaviour. As such, it is implausible that the biological mechanisms involved would be specific for reading. Reading has not existed in the human behavioural repertoire long enough for this to take place. Instead, reading engages a set of neurocognitive dimensions, implemented through a distributed network of areas in the brain, each of which contributes to the information processing required for reading, but none capturing reading behaviour in its entirety. Reading in the brain is therefore implemented through a functional network of discrete brain areas, none of which is uniquely endowed for this task22. Reading is a learned behaviour; it must be taught. Therefore, reading expertise at a neural level is achieved by the refinement of the functional coupling of these distributed areas that contribute to the task of reading, to form emergent neural networks.
Neuroscience now understands that the basic neural network for implementing reading involves at least three main processing hubs, normally lateralised within the left hemisphere of the brain23-25. It is now widely accepted that successful reading requires the development, coordination and lateralisation of the function of at least these three key cortical areas, in the left inferior temporal cortex, temporo-parietal cortex and inferior frontal gyrus, with processing in the hubs corresponding generally to the extraction of orthographic, phonological and semantic information from printed words, respectively26,27. What research studies have shown us is the close correspondence between the components of reading predicted by existing cognitive models27-29 and the engagement of these different brain areas under different task conditions. See Figure 2.
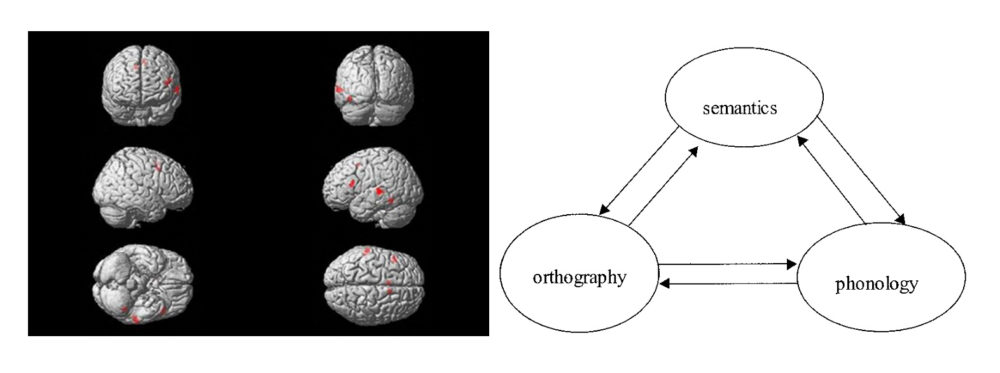
Figure 2. Left panel; A simplified neural network for reading comprised of three main hubs, lateralised to the left hemisphere. Images acquired during the learning of a second written language, for a word-pseudoword lexical decision task. Real words or unpronounceable letter strings were presented, following which an appropriate button was pressed on a response pad. The resulting images show the difference in blood oxygen level (‘BOLD’) between the word and pseudoword conditions; areas shown in red represent those in which blood oxygenation was higher in the word condition, compared to that for pseudowords, at a pre-defined statistical threshold. Right panel, a schematic of a cognitive model of reading based on computer simulations, showing the interactive and recursive relationships between orthography, phonology and semantic processing for the understanding of written words.
As previously outlined, dyslexia is typically characterised by persistent difficulties in achieving reading accuracy and fluency at the level of proficiency that would be expected from an individual’s age and profile of other abilities. A body of prior work has demonstrated neurophysiological differences in each of the three main hubs of the reading network, mostly using functional neuroimaging techniques that measure metabolic changes associated with the increased local demands on energy that result from relevant stimulus processing (for reviews see30-32) and including altered functional coupling between the main areas in this default reading network33,34. While these differences in the brains of dyslexic readers may also result from their poorer reading efficiency, there is also evidence of developmentally mediated structural differences in these brain areas both in grey and in white matter, that would be expected to precede and mediate functional differences in their activity patterns35-38.
Given that the brain is closer to the site of gene function than is measured behaviour, we can begin to ask questions about how brain phenotypes resulting from such genetic influences emerge and work to constrain reading development, or act as dimensional variables to modulate the probability of dyslexia risk (See Figure 1). Because both reading accuracy and fluency, and associated component skills in orthographic, phonological and semantic processing are all significantly heritable39, a platform of genetic research has been conducted to identify the extent to which gene associations with different reading components, or which differ across groups of dyslexia and of typical readers40, are linked to variables associated with their brain development41. Since the completion of the Human Genome project in 200342, scientists are now been able to analyse genetic variability across the entire human genome, for comparisons across individuals and/or groups. To date, there are at least nine reported candidate regions of interest for dyslexia across the human genome and at least 14 individual candidate genes43. As with all of the dyslexia risk genes so far discovered, the targeted genes are expressed in the brain and impact upon neurodevelopment in at least two main ways: 1. through the way in which neurons connect with one another (structural and functional connectivity) in the formation of neural networks; 2. by influencing neurodevelopment more generally through modifying its structure in pre-natal and early childhood development44-46.
Summary
Educational practice is validated through behavioural observations of children’s achievement. These observations can be either objective or based on subjective impressions of children’s attainment of developmental milestones. Current assessment practice of children’s academic strengths and difficulties is particularly effective in identifying individual children who would benefit from structured interventions to improve or augment their achievement in particular skill domains. What this practice copes with less well, however, is the ability to identify and validate clusters of children with similar patterns of underlying deficits, particularly those in cognitive processing and neurobiology that underpin both typical and atypical development. As applied to children’s learning, understanding the underpinning neuroscience and how changes manifest across development holds particular promise in achieving more valid taxonomies that adequately identify and characterise these children.
Dimensional frameworks appear to capture the nature of the underlying genetic, neurological and cognitive risk factors, which likely modify risk for dyslexia as continuous variables, and therefore confer risk through probabilistic more than deterministic mechanisms. Such risk models appear particularly well-suited to identifying and characterising the changing profiles of developmental disorders over time, and in the context of high intra-individual variability in the relevant risk dimensions. On advancing this framework, single deficit accounts of dyslexia will be emphasised less, in favour of frameworks that better acknowledge the individual variability within the risk factors involved, and the highly overlapping nature of dyslexia with other disorders of learning.
References
- Shaywitz, S.E., Escobar, M.D., Shaywitz, B.A., Fletcher, J.M., & Makuch, R. (1992). Evidence that dyslexia may represent the lower tail of a normal distribution of reading ability. New Engl J, 326, 145–150. https://doi.org/10.1056/NEJM199201163260301
- Snowling, M.J., & Hulme, C. (2012). Annual research review: The nature and classification of reading disorders – A commentary on proposals for DSM-5. J Child Psychol Psychiatry, 53, 593–607. https://doi.org/10.1111/j.1469-7610.2011.02495.x
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (fifth edition). American Psychiatric Association.
- Elliot, J. (2020). It’s time to be scientific about dyslexia. Read Res Q, 55, 61–75.
- Elliott, J., & Grigorenko, E.L. (2014). The dyslexia debate. Cambridge University Press.
- Pringle-Morgan, W.P. (1896). A case of congenital word blindness (inability to learn to read). Br Med J, ii, 1533–1544.
- Peterson, R.L., & Pennington, B.F. (2015). Developmental dyslexia. Ann Rev Clinl Psychol, 11, 283–307.
- Peterson, R.L., & Pennington, B.F. (2012). Developmental dyslexia. Lancet, 26, 1997–2007.
- Wagner, R.K., et al. (2020). The prevalence of dyslexia: A new approach to its estimation. J Learn Disabil, 53, 354–365.
- Astle, D.E., Holmes, J., Kievit, R., & Gathercole. (2021). S.E. Annual Research Review: The transdiagnostic revolution in neurodevelopmental disorders. J Child Psychol Psychiatr. https://doi.org/10.1111/jcpp.13481
- Cuthbert, B.N., & Insel, T.R. (2013). Toward the future of psychiatric diagnosis: The seven pillars of RDoC. BMC Med, 11, 126.
- R-Mercier, A., Masson, M., Bussières, E.L., & Cellard C. (2018). Common transdiagnostic cognitive deficits among people with psychiatric disorders exposed to childhood maltreatment: A meta-analysis. Cogn Neuropsychiatry, 23, 180–197.
- Reininghaus, U., et al. (2019). Transdiagnostic dimensions of psychosis in the Bipolar‐Schizophrenia Network on Intermediate Phenotypes (B‐SNIP). World Psychiatry, 18, 67–76.
- Casey, B.J., Oliveri, M.E., & Insel, T. (2014). A neurodevelopmental perspective on the Research Domain Criteria (RDoC) framework. Biological Psychiatry, 76, 350–353.
- Talcott, J.B., Witton, C., & Stein, J.F. (2013). Probing the neurocognitive trajectories of children’s reading skills. Neuropsychologia, 51, 472–481.
- Morton, J., & Frith, U. (1995). Causal modeling: A structural approach to developmental psychopathology. In D. Cicchetti & D.J. Cohen (Eds.), Wiley series on personality processes. Developmental psychopathology, Vol. 1. Theory and methods (p. 357–390). John Wiley & Sons.
- Beaton, A. (2004). Dyslexia, reading and the brain: A sourcebook of psychological and biological research. Psychology Press.
- Høien, T., & Lundberg, I. (2000). Dyslexia: From theory to intervention. Kluwer Academic Publishers.
- Nicolson, R.I., & Fawcett, A.J. (2008). Dyslexia, learning and the brain. MIT Press.
- Snowling, M.J. (2000). Dyslexia (2nd edn). Blackwell.
- Pennington, B.F. (2006). From single to multiple deficit models of developmental disorders. Cognition, 101, 385–413.
- Dehaene, S. (2009). Reading in the brain: The new science of how we read. Penguin
- Turkeltaub, P.E., Eden, G.F., Jones, K.M., & Zeffiro, T.A. (2002). Meta-analysis of the functional neuroanatomy of single-word reading: Method and validation. Neuroimage, 16, 765–80.
- Murphy, K.A., Jogia, J., & Talcott, J.B. (2019). On the neural basis of word reading: A meta-analysis of fMRI evidence using activation likelihood estimation. J Neurolinguistics, 49, 71–83.
- Price C.J. (2012). A review and synthesis of the first 20 years of PET and fMRI studies of heard speech, spoken language and reading. NeuroImage, 62, 816–847.
- Frost, S.J., et al. (2005). A functional magnetic resonance imaging study of the tradeoff between semantics and phonology in reading aloud. Neuroreport, 16, 621–624.
- Seidenberg, M.S. (2005). Connectionist models of word reading. Current Directions in Psychological Science, 14, 238–242.
- Harm, M., & Seidenberg, M.S. (1999). Reading acquisition, phonology, and dyslexia: Insights from a connectionist model. Psychological Review, 106, 491–528.
- Plaut, D.C., McClelland, J.L., Seidenberg, M.S., & Patterson, K. (1996). Understanding normal and impaired word reading: Computational principles in quasi-regular domains. Psychological Review, 103, 56–115.
- Maisog, J.M., Einbinder, E.R., Flowers, D.L., Turkeltaub, P.E., & Eden, G.F. (2008). A meta-analysis of functional neuroimaging studies of dyslexia. Ann. N. Y. Acad. Sci, 1145, 237–259.
- Richlan, F., Kronbichler, M., & Wimmer. H. (2009). Functional abnormalities in the dyslexic brain: a quantitative meta-analysis of neuroimaging studies. Hum. Brain Mapp, 30, 3299–3308.
- Démonet, J.F., Taylor, M.J., & Chaix, Y. (2004). Developmental dyslexia. Lancet, 363, 1451–1460.
- Pugh K.R., Mencl W.E., Shaywitz B.A., et al. (2000). The angular gyrus in developmental dyslexia: Task-specific differences in functional connectivity within posterior cortex. Psychological Science, 11(1), 51–56. https://doi.org/10.1111/1467-9280.00214
- Finn, E.S., et al. (2014). Disruption of functional networks in dyslexia: A whole-brain, data-driven analysis of connectivity. Biological Psychiatry, 76, 397–404.
- Vogel, A.C., et al. (2013). Functional network architecture of reading-related regions across development. Brain and Language, 125, 231–243.
- Black, J.M., Xia, Z., & Hoeft, F. (2017). Neurobiological bases of reading disorder Part II: The importance of developmental considerations in typical and atypical reading. Lang Linguist Compass, 11, e12252
- Silani, G., et al. (2005). Brain abnormalities underlying altered activation in dyslexia: A voxel based morphometry study. Brain, 128, 2453–2461.
- Beaulieu, C., et al. (2005). Imaging brain connectivity in children with diverse reading ability. NeuroImage, 25, 1266–1271.
- Gayan, J., & Olson, R.K. (2003). Genetic and environmental influences on individual differences in printed word recognition. J Exp Child Psychol, 84, 97–123.
- Fisher, S.E., & DeFries, J.C. (2002). Developmental dyslexia: Genetic dissection of a complex cognitive trait. Nat Rev Neurosci, 3, 767–780.
- Eicher, J.D., & Gruen, J.R. (2013). Imaging-genetics in dyslexia: connecting risk genetic variants to brain neuroimaging and ultimately to reading impairments. Molecular genetics and Metabolism, 110, 201–212.
- The Human Genome Project. https://www.genome.gov/human-genome-project
- Carrion-Castillo, A., Franke, B., & Fisher, S.E. (2013). Molecular genetics of dyslexia: an overview. Dyslexia, 19(4), 214–240.
- Poelmans, G., Buitelaar, J.K., Pauls, D.L., & Franke B. (2011). A theoretical molecular network for dyslexia: integrating available genetic findings. Mol Psychiatry, 16, 365–382.
- Paracchini, S., et al. (2006). The chromosome 6p22 haplotype associated with dyslexia reduces the expression of KIAA0319, a novel gene involved in neuronal migration. Hum Mol Genet, 15, 1659–1666.
- Guidi, L.G., et al. (2018). The neuronal migration hypothesis of dyslexia: A critical evaluation 30 years on. Eur J Neurosci, 48, 3212–3233.