Neural and behavioral correlates of child maltreatment in the context of education

Executive Summary
- All children have the right to be protected from violence, yet child maltreatment is a pervasive problem worldwide
- Teachers play a crucial role in recognizing and reporting maltreatment
- Maltreatment affects the development of both behavior and the brain
- The developing brain may be shaped by the abusive environment to process information differently across many domains (for example, executive function, error, reward, and socioemotional processing)
- Neural adaptations that are useful in an abusive environment may not be useful in classroom learning
Introduction
The right of all children to be protected from all forms of violence is recognized in international human rights treaties. For example, Article 19 of the UN Convention on the Rights of the Child states that all Parties “shall take all appropriate legislative, administrative, social and educational measures to protect the child from all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse”1. And yet children still suffer physical, sexual, and emotional abuse and neglect around the world.[1] Globally, it has been estimated that 1 billion 2- to 17-year-olds experience such violence in a given year2.
[1] The terms “abuse and neglect” and “maltreatment” are used interchangeably in this brief.
The crucial roles of teachers
In some countries (including the United States), teachers, guidance counselors, school administrators, and staff are mandated to report suspected cases of child abuse to child protective service agencies. According to federal data, education personnel in the United States are the primary reporting source of suspected child maltreatment, as shown in Figure 13. Indeed, education professionals report cases that would have been missed otherwise and thus play a key role in identifying children in need of services4. Why are parents not reporters? Unfortunately, federal data from the United States indicate that parents are the perpetrators of maltreatment in almost 92% of cases3, Table 3-11, p. 44.
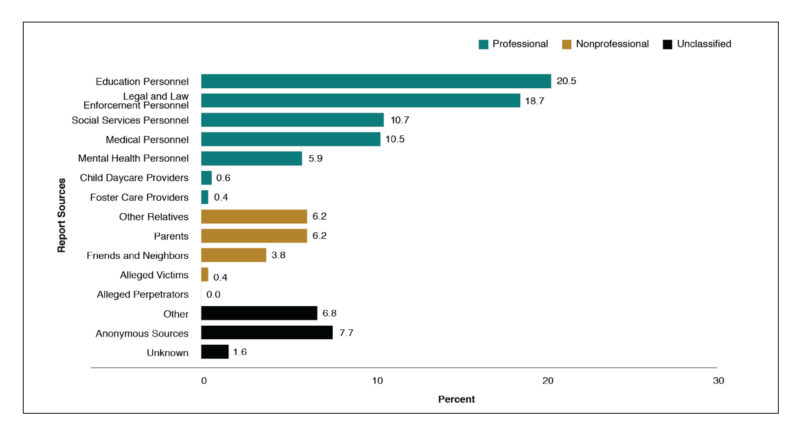
Figure 1. The most recent (2018) data from the United States indicate that education personnel are responsible for the greatest percentage of reported allegations of child maltreatment. From ref 3, Exhibit 2-D, p. 9.
Although teachers are mandatory reporters in some countries, their knowledge, training, attitudes, and work experience all influence their decisions to reporte.g., 5,6-9. Studies have indicated that teachers may need further training on maltreatment reporting laws, what constitutes abuse, how to report abuse, or signs of abuse across many countries, including Australia10,11, Belgium12, Canada13,14, Estonia15, India16, Ireland17, Jordan18, Singapore19, Turkey20,21, and the United States22-25. More consistent and higher-quality training of education professionals would likely lead to more effective reporting and increased ability to help children and families4.
Training can also help teachers become aware of the impacts of childhood trauma related to maltreatment26. As part of a team of caring adults in a child’s life, teachers can provide trauma-informed education for their students, building reliable relationships and providing supportive, predictable, and safe environmentse.g., 26,27,28,29. Trauma-informed education typically focuses on helping children to learn or rebuild socioemotional, self-regulation, and relationship skills30. It can also focus on strengths, such as what psychological resources the child already has that can be built on for successe.g., 31,32. There are multiple guides for developing trauma-informed classrooms and schoolse.g., 28,33,34, but little evidence of efficacy. Although classroom teachers are generally not certified to provide mental health treatment (see Appendix), they can provide socioemotional support and understand and accommodate the range of learning challenges that children who have been maltreated may have.
Potential long-term effects of maltreatment
Studies of adverse childhood experiences, such as maltreatment, have reported mental health, physical health, behavioral, and social consequences well into adulthoode.g., 35,36,37. See Figure 2. For example, children who have experienced abuse or neglect are more likely to have depression and diabetes as adults, to have difficulties with relationships, to struggle with substance abuse, and to be involved in violence and criminal behaviore.g., 38,39-41. How are these lifelong outcomes related to early experiences of adversity? One mechanism is through the pervasive effects of toxic stress on the brain and body (e.g., https://developingchild.harvard.edu/science/key-concepts/toxic-stress/). Greater exposure to adverse childhood experiences is associated with greater risk of poor outcomes42. However – importantly – individual, family, and community factors interact to influence these outcomes: Many children develop resilience43 that protects against these effects (see the brief in this series Resilience for lifelong learning and well-being).
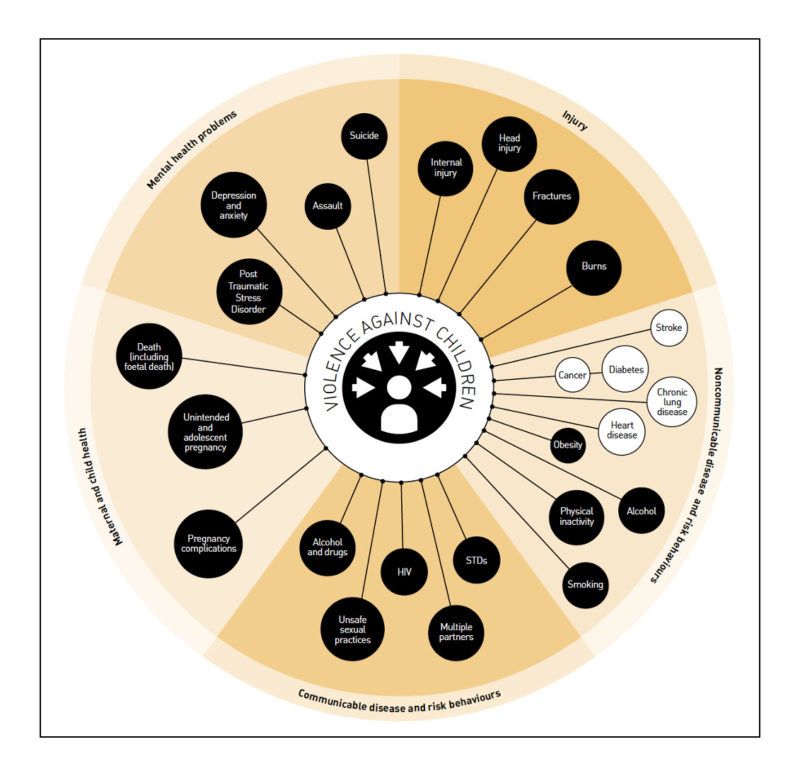
Figure 2. The long-term effects of maltreatment can be extensive and include both direct effects (dark circles) and indirect effects due to the adoption of high-risk behaviors (white circles). From ref 36, Figure 1: Potential health consequences of violence against children, p. 11. Reproduced with permission from WHO from INSPIRE: seven strategies for ending violence against children, https://www.who.int/publications/i/item/inspire-seven-strategies-for-ending-violence-against-children, © 2016.
Child maltreatment can also have enduring economic effects. Adults with a history of maltreatment have lower levels of employment, lower earnings, and fewer assets44. At a societal level, the total lifetime economic burden resulting from new cases of maltreatment in 2008 in the United States was estimated at $124 billion, ranging to $585 billion in further sensitivity analyses45.
Globally, violence in childhood is also associated with educational outcomes, including increased risk of school drop-out and poorer academic performance46. In the United States, even by the third grade, children who have been involved with child protective services score significantly lower on standardized math and reading tests, are more likely to be identified as needing special education, and are more likely to be held back a grade47. The next section takes a closer look at some of the learning differences that children who have been maltreated may have.
Potential near-term effects of maltreatment: neural and behavioral correlates of maltreatment in the classroom[2]
One of the key developmental features of the human brain is neuroplasticity. The brain grows and changes in interaction with the environment. Both the physical structure and the functioning of the brain are shaped by our experiences (in interaction with our genes). When those experiences involve maltreatment, the brain develops to adapt to the abusive or neglectful environment in which a child is growing upe.g., 49,50-54. However, adaptations that support survival in the maltreating environment may not support successful learning in the classroom environment.
The focus of this section is classroom-relevant skills that have been investigated in functional neuroscience studies with children who have been maltreated. More extensive reviews of the structural and functional neural correlates of maltreatment in children and adults are available elsewheree.g., 48,54,55,56-71. It is important to remember that these are correlational findings72 and that many children are resiliente.g., 73. Thus, not every maltreated child will have the same pattern of strengths and weaknesses.
Overall, research suggests that many kinds of processing develop differently in children who have experienced maltreatment. Some findings indicate that maltreatment affects two neural networks in particular: one involved in executive functions (a fronto-striatal system) and another involved in emotion and motivation processing (a fronto-limbic system), as illustrated in Figure 3e.g., 48. Thus, maltreatment can have pervasive effects on neural systems that are fundamental for learning and development.
[2] Note that ethical research with this vulnerable population is challenging and that there are limitations to this literature such as small sample sizes and failure to control for confounding factors like comorbid psychiatric diagnosese.g., 48. Also note that the general effects of stress on learning are not addressed here, as they are addressed in other briefs in this series.
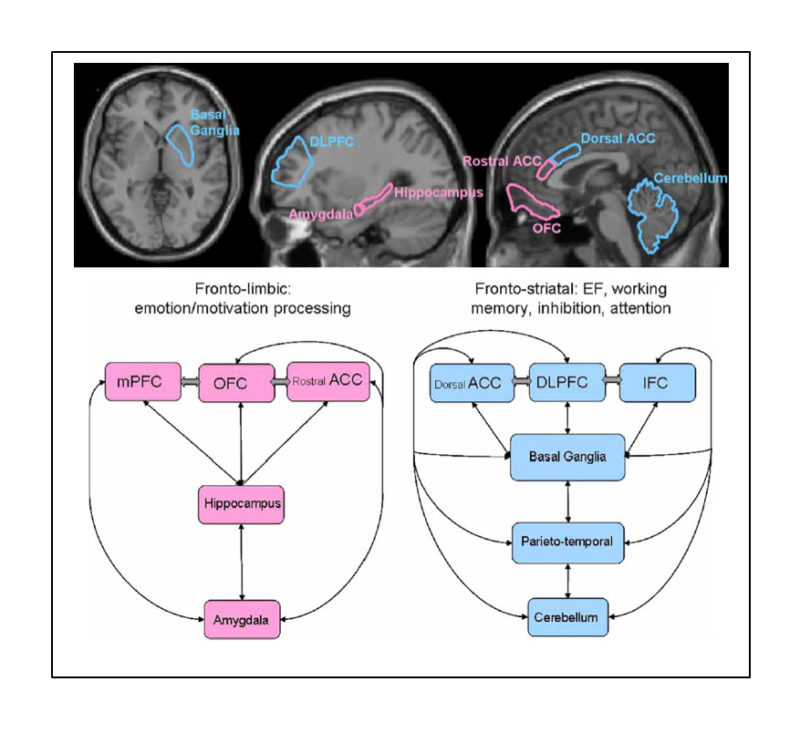
Figure 3. Neuroscience evidence suggests different processing in a fronto-limbic system involved in emotion and motivation (pink) and a fronto-striatal system involved in executive functioning (blue) in children and adolescents who have experienced maltreatment. From ref 48, Hart & Rubia, 2012, Neuroimaging of child abuse: a critical review; Figure 1, p. 8, and Figure 2, p. 17, combined. Used under CC-BY 4
Executive functions
Behavioral studies with children and adolescents with a history of maltreatment have shown that many executive functions, such as working memory, inhibitory control, sustained attention, cognitive flexibility, and processing speed, develop differently in this populatione.g., 68,74,75-88. Poorer executive functioning likely influences the poorer academic performance of children who have been maltreated89. In the following paragraphs, we consider why.
How is working memory used in the classroom? Anything that requires children to keep information “in mind” requires working memory. For example, instructions (get your math books, turn to page 19, and complete all of the odd-numbered problems before noon), reading comprehension (remembering what you have just read and connecting that to what you are now reading), and remembering a teacher’s question while trying to come up with an answer all rely on working memory. Consistent with behavioral evidence of poorer working memory in children who have been maltreated, a neuroimaging study reported that 8- to 19-year-olds with a history of maltreatment and exposure to violence showed different activation in a frontoparietal network that supports working memory, in comparison to nonmaltreated controls90. Processing differences for the working memory task were seen during both encoding (getting information into memory) and retrieval (recalling, or getting information back out of memory)90.
What does inhibitory control look like in a classroom? You might think of it as poor impulse control. Consider blurting out an answer without raising a hand, even before the question has been completed. Or saying what comes to mind without stopping to think first. And consider what effects these sorts of behaviors have on peer relationshipse.g., 91,92. Consistent with behavioral findings of poorer inhibitory control in children who have been maltreated, neuroimaging studies have shown that children and adolescents with a history of maltreatment, in comparison to peers without a history of maltreatment, show different patterns of activity in a fronto-striatal network associated with inhibitory and response control during tasks requiring these skills93-96.
Why is attention important in the classroom? Attention is required to get information into memory and learn it, by focusing on important information (for example, what the teacher is saying) and tuning out unimportant information (for example, the whispers of classmates). A child who is attending to their own anxiety, the shadow of a figure at the classroom door, or a personal memory cannot also sustain attention to the teacher or a peer’s question. A child who seems lost or confused and cannot keep up with academic activities or daily classroom rhythms may be struggling with attention. Consistent with the results of behavioral studies indicating poorer sustained attention in children who have been maltreated, neuroimaging studies have found that adolescents who have experienced severe childhood abuse, as compared to controls who have not, make more errors on attention tasks, show less connectivity in frontoparietal attention networks, and show reduced activation in frontal attention regions during sustained attention tasks97,98.
Increased sensitivity to error
In some neuroimaging studies, adolescents with a history of childhood abuse have been asked to perform a task designed to elicit mistakese.g., 99,100. These studies found increased activation but less connectivity in the fronto-cingulo-striatal network involved in error processing in the adolescents who had been maltreated, in comparison to nonmaltreated controls99,100. These differences were limited to processing of mistakes: For correct responses, there were no differences between the two groups99,100. Other neuroimaging studies have also reported more neural resources allocated to error processing – a hypersensitivity to errors – in children who have been maltreated101.
Further, a brainwave recording study with 6-year-olds also used a task designed to elicit mistakes102. As illustrated in Figure 4, a specific neural response associated with recognizing that one has made an error (the error-related negativity) was larger in children who had experienced more hostile parenting, as compared to children raised in more responsive families102. That is, children who had experienced more harsh parenting devoted more neural resources to recognizing and processing their own mistakes on the task. These children were not identified as maltreated. Hostile (harsh, punitive) parenting was defined in terms of parental expressions of anger, frustration, and criticism toward the child during a structured visit to the research laboratory when the children were three years old102, p. 823.
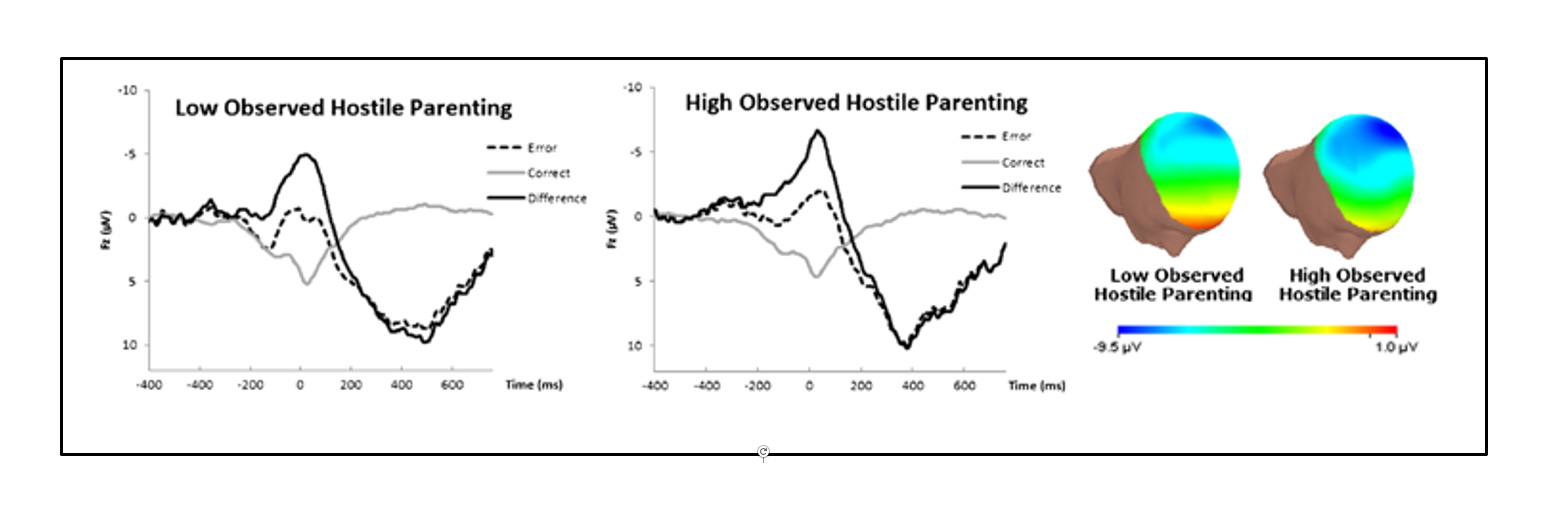
Figure 4. Left: Brainwaves to correct (gray line) and error (dashed black line) responses, as well as the mathematical difference between the two types of responses (solid black line) for children growing up with parents rated low and high in terms of hostile parenting style. Right: The difference data plotted as topographic maps; the deeper blue and greater extent of blue for children with parents rated high on hostile parenting style indicates the larger error-related negativity in this group – that is, the greater neural response to realizing that one has made a mistake. From ref 102, Figure 1, p. 826. Reprinted by permission from Springer Nature: Springer, Journal of Abnormal Child Psychology, Self-reported and observed punitive parenting prospectively predicts increased error-related brain activity in six-year-old children, A. Meyer, G.H. Proudfit, S.J. Bufferd, A.J. Kujama, R.S. Laptook, D.C. Torpey, & D.N. Klein, © 2014.
Increased sensitivity in error detection and processing networks in children and adolescents who have been maltreated may be due to the “constant need to monitor their own actions in order to avoid painful mistakes, which are often associated with harsh punishment in abusive settings”100, p. 892. That is, the consequences of making a mistake may be particularly salient. Hypersensitivity to errors may be a useful adaptation for an abusive environment, but maladaptive for a school environment. What might it look like in a classroom? Perhaps a math worksheet that is erased over and over and never turned in for fear of mistakes. Perhaps a child “freezing” the moment they recognize that they have made a mistake. Perhaps an unexpected over-reaction to a gentle suggestion that a student check their work.
Reward processing
A number of behavioral studies have reported decreased sensitivity to reward in children who have experienced maltreatmente.g., 103,104,105. For example, in one study, 8- to 14-year-olds with a history of abuse did not change their response speed based on the likelihood of a reward, whereas children without a history of abuse responded more quickly as the chances of winning a reward increased103. In another study, 12- to 17-year-olds who had been exposed to physical abuse were less able than their nonabused peers to learn which stimuli were likely to result in reward, even after repeated feedback105. Less use of information about rewards may be related to the variability in how abusive caregivers respond to children105. Thus, assuming that positive feedback and rewards are not consistent or reliable may be an adaptation that children develop in an abusive context105, p. 776 that is counterproductive for learning in the classroom.
In accord with the behavioral findings, a history of maltreatment has been associated with reduced activation in the reward network in neuroimaging studiese.g., 101,106,107. For example, as shown in Figure 5, maltreatment experience was associated with reduced activation to reward cues in a study with 10- to 15-year-olds101.
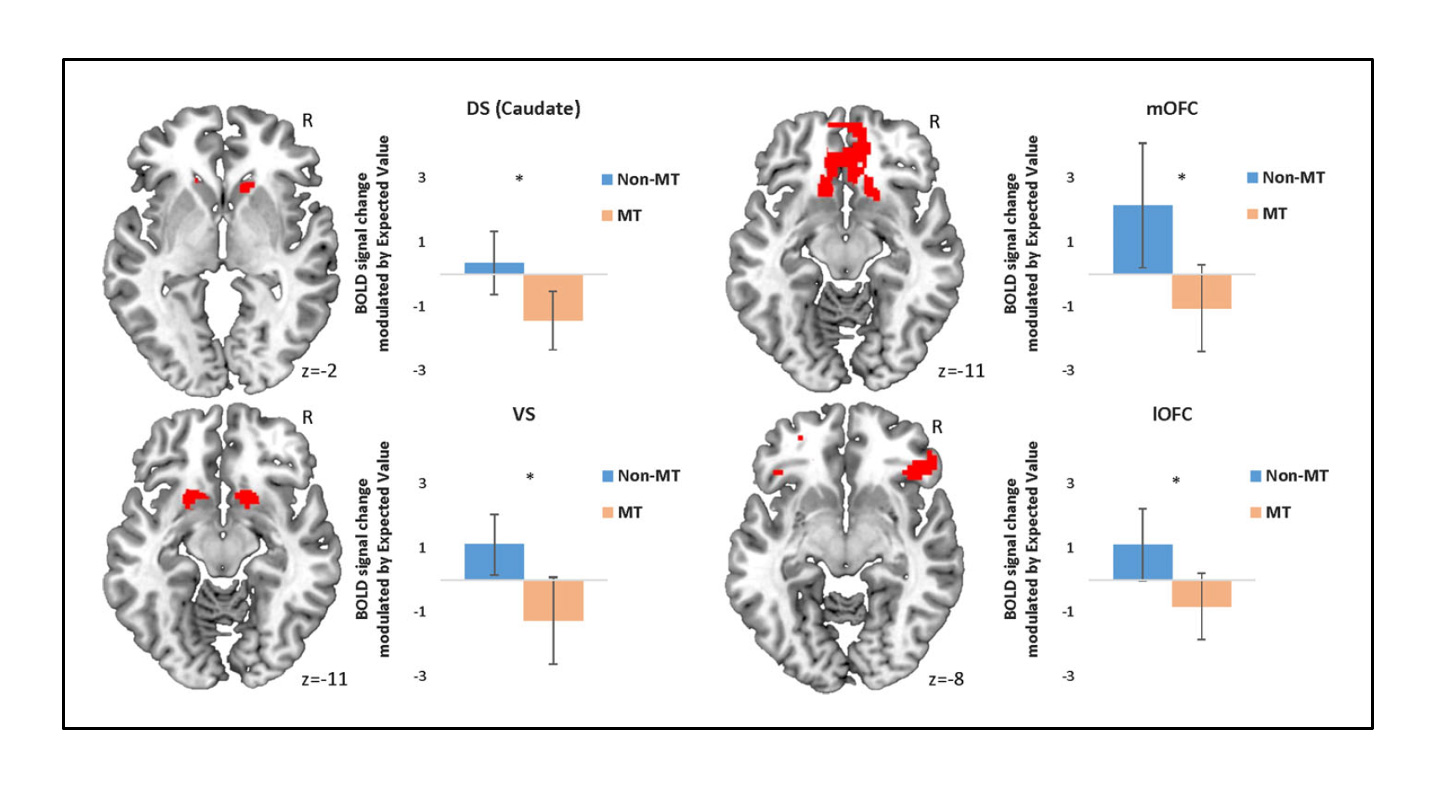
Figure 5. Reduced activation during reward processing in children and adolescents with a history of maltreatment (orange bars) in comparison to children and adolescents without a history of maltreatment (blue bars). Activation levels were modulated by expected reward (value) during avoidance responses in the dorsal striatum of the caudate (DS), the ventral striatum (VS), and the medial (mOFC) and lateral (lOFC) orbitofrontal cortex. From ref 101, Figure 3, p. 1698. Gerin et al., 2017, A neurocomputational investigation of reinforcement-based decision making as a candidate latent vulnerability mechanism in maltreated children. Used under CC-BY 4
Again, reduced responses to anticipated rewards may be learned from a negative environment in which rewards are unpredictable and scarcee.g., 63,105. They may also reflect an adaptive response in a dangerous environment that “tip[s] the balance in an approach-avoidance conflict situation to avoidance”54, p. 254. That is, children who have been abused may have learned not to engage; they may be motivated to avoid and disengage (especially from potential conflict) for survival in an abusive environment. What might this look like in the classroom? Perhaps a child who is not motivated by reward, avoids engagement even when rewards are involved, or may not respond positively when rewards are given.
Emotion processing
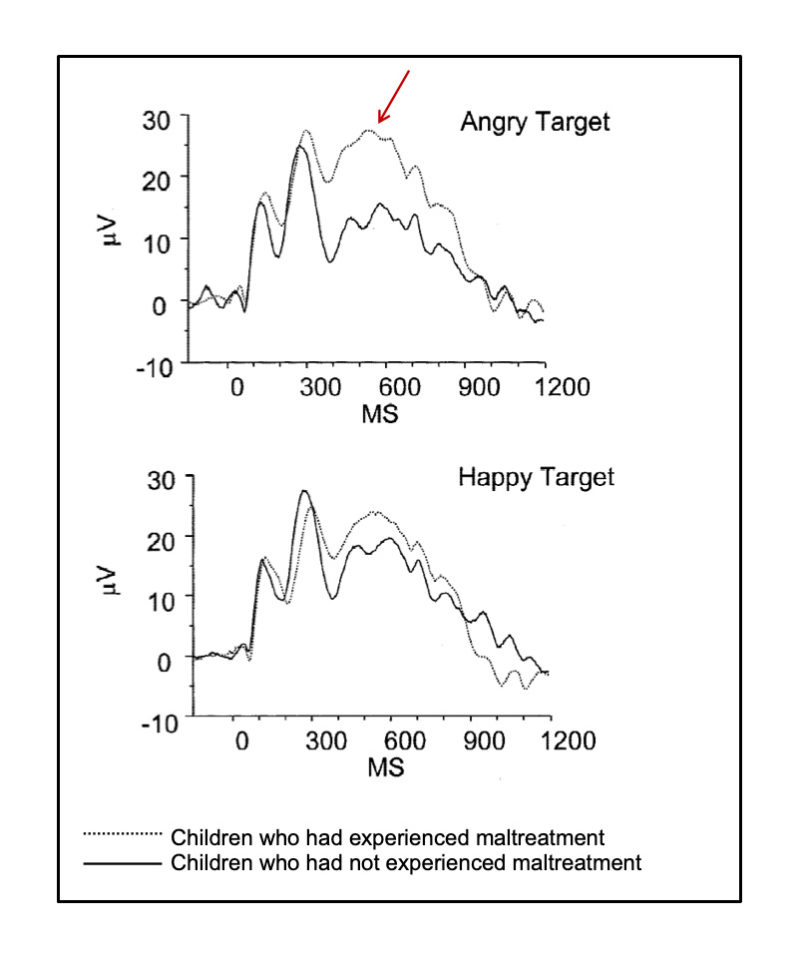
Figure 6. Children who have been maltreated show heightened sensitivity to (and devote more processing resources to) angry faces, as compared to children who have not been maltreated (see red arrow). In this study with 6- to 12-year-olds, the two groups processed happy faces similarly. Adapted from ref 121, Figure 3, p. 272. Pollak, Klorman, Thatcher, & Cicchetti, 2001, P3b reflects maltreated children’s reactions to facial displays of emotion. Used with permission of Wiley/Society for Psychophysiological Research (U.S.).
Behavioral research has shown that children who have been maltreated respond to emotional information differently than children who have not been maltreated108,109. Young children who have been maltreated are less accurate at identifying and discriminating between emotional facial expressionse.g., 110,111,112. They may have less emotion knowledge overall113, but may also have specialized emotion knowledge. For example, in one study, children who had been neglected had a lower standard for selecting sad faces and children who had been physically abused had a lower standard for selecting angry faces112. Indeed, many studies have reported more sensitivity and attention to angry facial expressions in children who have been physically abusede.g., 114,115-117. Overall, the pattern of results suggests that children who have been maltreated pay more attention to threatening emotional cues (like angry facial expressions)108.
In brainwave recording studies, infants as young as 15 months old, toddlers, and children who have been maltreated show greater responses to faces with angry expressions than other emotionse.g., 115,118-122. This is illustrated in Figure 6121. Children who have been physically abused also over-attend to visual and auditory anger cuese.g., 123,124. Overall, this pattern indicates allocation of more processing resources to threatening information; in turn, this can undermine attentional controle.g., 121,122. That is, focusing attention on monitoring for threatening cues may support survival in abusive situations but may interfere with shifting attention toward emotional regulation e.g., 125, a more adaptive response in the classroom.
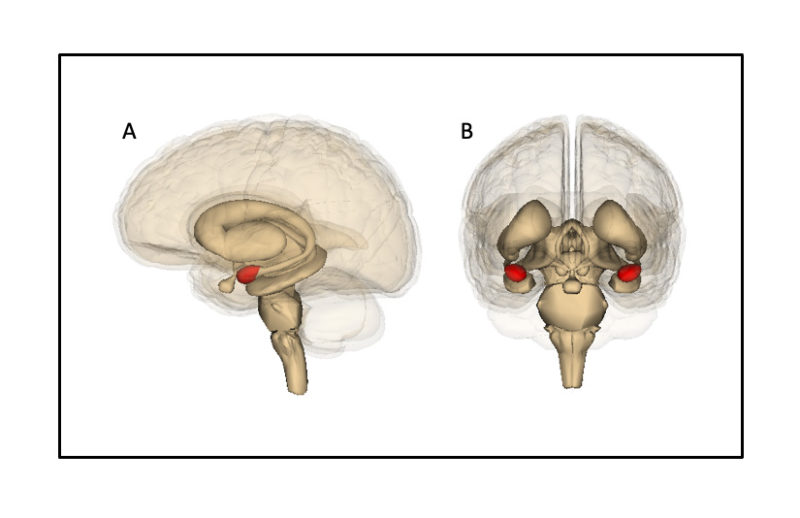
Figure 7. The amygdala (shaded red) as seen (A) from the side (left amygdala) and (B) from the front (left and right amygdalae). The amygdala is involved in emotion and fear processing. Life Science Databases(LSDB)/Wikimedia Commons, CC BY-SA 2.1 JP
Neuroimaging studies have also found that children and adolescents with a history of maltreatment respond faster to threatening information and show enhanced activation during fear or threat perception, as compared to nonmaltreated controlse.g., 126,127-134. Adolescents with histories of trauma also show greater amygdala (see Figure 7) reactivity to emotional conflict (for example, the word fear superimposed on a happy face) than controls135. Greater amygdala activation to angry as compared to neutral faces in adolescents with a history of maltreatment in comparison to controls has been observed even when the faces were presented outside of conscious awareness130. This suggests that some part of altered socioemotional processing toward threat may not be under conscious control.
However, remarkably, children and adolescents with a history of maltreatment are able to decrease their responses (down-regulate amygdala activation) to negative images (through a process called reappraisal) to a similar degree as nonmaltreated controls133,134. They just have to recruit more neural processing resources to do so133,134. Considering a different kind of resource, the availability and extent of social support may also moderate the heightened response to threat in children and adolescents with a history of maltreatment136.
Expertise at processing threat information “makes what is adaptive within an abusive environment maladaptive in more normative social settings”122, p. 371. What might this look like in a classroom? Perhaps monitoring of a teacher’s face and movements for any sign of anger or threat, to the detriment of listening to and learning what the teacher is saying. Or instantly mis-interpreting the accidental bump of a classmate in a busy hallway as threatening. It is likely that this pattern of socioemotional information processing55 is related to the enduring social difficulties of many children who have experienced maltreatment137,138.
Conclusion
Overall, this research provides a deeper understanding of how children who have been maltreated might process information differently, and why. This understanding may help teachers and school leaders to identify these children, better support them as learners, and reflect on their relationships with them. Both the neural and behavioral evidence suggests that maltreating environments can shape the brains of children to process information differently, in ways that may be adaptive in the abusive environment but not beneficial in the classroom environment.
With this knowledge, teachers might, for example, learn to reinterpret challenging behaviors as effects of trauma rather than willful noncompliance. In turn, educators might respond to such behaviors by “seek[ing] out therapeutic and positive behavioral supports, rather than responding with punitive measures such as suspensions or expulsions”28, p. 6. Exclusionary discipline serves no purpose for these children: It both robs them of opportunities to learn in a positive classroom environment and may require them to spend more time in the negative abusive environment, in addition to potentially being a triggering event for additional maltreatment.
Finally, this research urges us to think differently about an exclusive focus on academic content in the classroom, and to recognize that there are additional important capacities that need to be nurtured for effective learning32, p. 611. If we aspire to achieve Sustainable Development Goal 4 (https://sdgs.un.org/goals/goal4), ensuring inclusive and equitable quality education for all, we must carefully consider our most vulnerable students – including those who have experienced maltreatment.
References
- UN General Assembly. Convention on the Rights of the Child. (New York, NY, 1989, 20 November).
- Hillis, S., Mercy, J., Amobi, A. & Kress, H. Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics 137, e20154079, doi:10.1542/peds.2015-4079 (2016).
- U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth, and Families & Children’s Bureau. Child maltreatment 2018. (U.S. Department of Health & Human Services, Washington, DC, 2020).
- Fitzpatrick, M. D., Benson, C. & Bondurant, S. R. Beyond reading, writing, and arithmetic: the role of teachers and schools in reporting child maltreatment. (National Bureau of Economic Research, Cambridge, MA, 2020).
- Ayling, N. J., Walsh, K. & Williams, K. E. Factors influencing early childhood education and care educators’ reporting of child abuse and neglect. Australasian Journal of Early Childhood 45, 95-108, doi:10.1177/1836939119885307 (2020).
- O’Toole, R., Webster, S. W., O’Toole, A. W. & Lucal, B. Teachers’ recognition and reporting of child abuse: a factorial survey. Child Abuse Negl. 23, 1083-1101, doi:10.1016/S0145-2134(99)00074-5 (1999).
- Walsh, K. & Farrell, A. Identifying and evaluating teachers’ knowledge in relation to child abuse and neglect: a qualitative study with Australian early childhood teachers. Teaching and Teacher Education 24, 585-600, doi:10.1016/j.tate.2007.07.003 (2008).
- Webster, S. W., O’Toole, R., O’Toole, A. W. & Lucal, B. Overreporting and underreporting of child abuse: teachers’ use of professional discretion. Child Abuse Negl. 29, 1281-1296 (2005).
- Gilbert, R. et al. Recognising and responding to child maltreatment. Lancet 373, 167-180, doi:10.1016/S0140-6736(08)61707-9 (2009).
- Goldman, J. D. G. & Grimbeck, P. Sources of knowledge of departmental policy on child sexual abuse and mandatory reporting identified by primary school student-teachers. Educational Review 63, 1-18, doi:10.1080/00131911003717220 (2011).
- Goldman, J. D. G. & Grimbeck, P. Preservice teachers’ sources of information on mandatory reporting of child sexual abuse. Journal of Child Sexual Abuse 24, 238-258, doi:10.1080/10538712.2015.1009607 (2015).
- Vanderfaeillie, J., De Ruyck, K., Galle, J., Van Dooren, E. & Schotte, C. The recognition of child abuse and the perceived need for intervention by school personnel of primary schools: results of a vignette study on the influence of case, school personnel, and school characteristics. Child Abuse Negl. 79, 358-370, doi:10.1016/j.chiabu.2018.02.025 (2018).
- Beck, K. A., Ogloff, J. R. & Corbishley, A. Knowledge, compliance, and attitudes of teachers toward mandatory child abuse reporting in British Columbia. Canadian Journal of Education 19, 15-29, doi:10.2307/1495304 (1994).
- Tite, R. Detecting the symptoms of child abuse: classroom complications. Canadian Journal of Education 19, 1-14, doi:10.2307/1495303 (1994).
- Toros, K. & Tiirik, R. Preschool teachers’ perceptions about and experience with child abuse and neglect. Early Childhood Education Journal 44, 21-30, doi:10.1007/s10643-014-0675-0 (2016).
- Khandagale, V. S. & Chavan, R. L. Child abuse and neglect: gender based teachers awareness. The International Journal of Indian Psychology 7, 113-121, doi:10.25215/0703.014 (2019).
- McKee, B. & Dillenburger, K. Child abuse and neglect: training needs of student teachers. International Journal of Educational Research 48, 320-330, doi:10.1016/j.ijer.2010.03.002 (2009).
- Fayez, M., Takash, H. M. & Al-Zboon, E. K. Combating violence against children: Jordanian pre-service early childhood teachers’ perceptions towards child abuse and neglect. Early Child Development and Care 184, 1485-1498, doi:10.1080/03004430.2014.901013 (2014).
- Briggs, F. & Potter, G. K. Singaporean early childhood teachers’ responses to myths about child abuse. Early Child Development and Care 174, 339-355, doi:10.1080/0300443032000153408 (2004).
- Kanak, M. & Avci, N. The effect of the training program to promote the knowledge and awareness of prospective preschool teachers on emotional neglect and abuse. Asian Journal of Education and Training 4, 137-145, doi:10.20448/journal.522.2018.42.137.145 (2018).
- Karadag, S. Ç., Sönmez, S. & Dereobali, N. An investigation of preschool teachers’ recognition of possible child abuse and neglect in Izmir, Turkey. Journal of Interpersonal Violence 30, 873-891, doi:10.1177/0886260514536274 (2015).
- Kenny, M. C. Child abuse reporting: teachers’ perceived deterrents. Child Abuse Negl. 25, 81-92, doi:10.1016/S0145-2134(00)00218-0 (2001).
- Kenny, M. C. Teachers’ attitudes toward and knowledge of child maltreatment. Child Abuse Negl. 28, 1311-1319, doi:10.1016/j.chiabu.2004.06.010 (2004).
- Reiniger, A., Robison, E. & McHugh, M. Mandated training of professionals: a means for improving reporting of suspected child abuse. Child Abuse Negl. 19, 63-69, doi:10.1016/0145-2134(94)00105-4 (1995).
- Smith, M. C. Early childhood educators: perspectives on maltreatment and mandated reporting. Children and Youth Services Review 32, 20-27, doi:10.1016/j.childyouth.2009.06.011 (2010).
- Substance Abuse and Mental Health Services Administration. SAMHSA’s concept of trauma and guidance for a trauma-informed approach. (Substance Abuse and Mental Health Services Administration, Rockville, MD, 2014).
- Crosby, S. D. An ecological perspective on emerging trauma-informed teaching practices. Children & Schools 37, 223-230, doi:10.1093/cs/cdv027 (2015).
- Cole, S. F., O’Brien, J. G., Gadd, M. G., Ristuccia, J. & Wallace, D. L. Helping traumatized children learn: supportive school environments for children traumatized by family violence. (Massachusetts Advocates for Children, Boston, MA, 2005).
- Crosby, S. D., Howell, P. & Thomas, S. Social justice education through trauma-informed teaching. Middle School Journal 49, 15-23, doi:10.1080/00940771.2018.1488470 (2018).
- Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D. & Schellinger, K. B. The impact of enhancing students’ social and emotional learning: a meta-analysis of school-based universal interventions. Child Dev. 82, 405-432, doi:10.1111/j.1467-8624.2010.01564.x (2011).
- Brunzell, T., Stokes, H. & Waters, L. Trauma-informed positive education: using positive psychology to strengthen vulnerable students. Contemporary School Psychology 20, 63-83, doi:10.1007/s40688-015-0070-x (2016).
- Brunzell, T., Stokes, H. & Waters, L. Shifting teacher practice in trauma-affected classrooms: practice pedagogy strategies within a trauma-informed positive education model. School Mental Health 11, 600-614, doi:10.1007/s12310-018-09308-8 (2019).
- Australian Childhood Foundation. Making space for learning: trauma informed practices in schools. (Australian Childhood Foundation, Ringwood, VIC, 2010).
- Wolpow, R., Johnson, M. M., Hertel, R. & Kinkaid, S. O. The heart of learning and teaching: compassion, resiliency, and academic success. (Washington State Office of Superintendent of Public Instruction, Olympia, WA, 2016).
- Felitti, V. J. et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am. J. Prev. Med. 14, doi:10.1016/j.amepre.2019.04.001 (1998).
- World Health Organization (WHO) et al. INSPIRE: seven strategies for ending violence against children. (WHO, Geneva, 2016).
- Child Welfare Information Gateway. Long-term consequences of child abuse and neglect. (Child Welfare Information Gateway, 2019).
- Gilbert, R. et al. Burden and consequences of child maltreatment in high-income countries. Lancet 373, 68-81, doi:10.1016/S0140-6736(08)61706-7 (2009).
- Norman, R. E. et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Medicine 9, e1001349, doi:10.1371/journal.pmed.1001349 (2012).
- Jonson-Reid, M., Kohl, P. L. & Drake, B. Child and adult outcomes of chronic child maltreatment. Pediatrics 129, 839-845, doi:10.1542/peds.2011-2529 (2012).
- Buckingham, E. T. & Daniolos, P. Longitudinal outcomes for victims of child abuse. Current Psychiatry Reports 15, 1-7, doi:10.1007/s11920-012-0342-3 (2013).
- Anda, R. F. et al. The enduring effects of abuse and related adverse experiences in childhood: a convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 256, 174-186, doi:10.1007/s00406-005-0624-4 (2006).
- Latham, R. M. et al. Development of an individualized risk calculator for poor functioning in young people victimized during childhood: a longitudinal cohort study. Child Abuse Negl. 98, 104188, doi:10.1016/j.chiabu.2019.104188 (2019).
- Currie, J. & Spatz Widom, C. Long-term consequences of child abuse and neglect on adult economic well-being. Child Maltreatment 15, 111-120, doi:10.1177/1077559509355316 (2010).
- Fang, X., Brown, D. S., Florence, C. S. & Mercy, J. A. The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse Negl. 36, 156-165, doi:10.1016/j.chiabu.2011.10.006 (2012).
- Fry, D. et al. The relationships between violence in childhood and educational outcomes: a global systematic review and meta-analysis. Child Abuse Negl. 75, 6-28, doi:10.1016/j.chiabu.2017.06.021 (2018).
- Ryan, J. P. et al. Early exposure to child maltreatment and academic outcomes. Child Maltreatment 23, 365-375, doi:10.1177/1077559518786815 (2018).
- Hart, H. & Rubia, K. Neuroimaging of child abuse: a critical review. Frontiers in Human Neuroscience 6, 1-24, doi:10.3389/fnhum.2012.00052 (2012).
- Cicchetti, D. Socioemotional, personality, and biological development: illustrations from a multilevel developmental psychopathology perspective on child maltreatment. Annu. Rev. Psychol. 67, 187-211, doi:10.1146/annurev-psych-122414-033259 (2016).
- McLaughlin, K. A., Sheridan, M. A. & Lambert, H. K. Childhood adversity and neural development: deprivation and threat as distinct dimensions of early experience. Neurosci. Biobehav. Rev. 47, 578-591, doi:10.1016/j.neubiorev.2014.10.012 (2014).
- McCrory, E. J. & Viding, E. The theory of latent vulnerability: reconceptualizing the link between childhood maltreatment and psychiatric disorder. Dev. Psychopathol. 27, 493-505, doi:10.1017/S0954579415000115 (2015).
- Pal, R. & Elbers, J. Neuroplasticity: the other side of the coin. Pediatr. Neurol. 84, 3-4, doi:10.1016/j.pediatrneurol.2018.03.009 (2018).
- Sheridan, M. A. & McLaughlin, K. A. Neurobiological models of the impact of adversity on education. Current Opinion in Behavioral Sciences 10, 108-113, doi:10.1016/j.cobeha.2016.05.013 (2016).
- Teicher, M. H. & Samson, J. A. Annual research review: enduring neurobiological effects of childhood abuse and neglect. Journal of Child Psychology and Psychiatry 57, 241-266, doi:10.1111/jcpp.12507 (2016).
- Bick, J. & Nelson, C. A. Early adverse experiences and the developing brain. Neuropsychopharmacology Reviews 41, 177-196, doi:10.1038/npp.2015.252 (2016).
- Bremner, J. D. Long-term effects of childhood abuse on brain and neurobiology. Child Adolesc. Psychiatr. Clin. N. Am. 12, 271-292, doi:10.1016/S1056-4993(02)00098-6 (2003).
- Carbrera, C., Torres, H. & Harcourt, C. The neurological and neuropsychological effects of child maltreatment. Aggression and Violent Behavior 54, 101408, doi:10.1016/j.avb.2020.101408 (2020).
- Carvalho, J. C. N. et al. Cognitive, neurobiological and psychopathological alterations associated with child maltreatment: a review of systematic reviews. Child Indicators Research 9, 389-406, doi:10.1007/s12187-015-9314-6 (2016).
- Glaser, D. Child abuse and neglect and the brain – a review. Journal of Child Psychology and Psychiatry 41, 97-116, doi:10.1111/1469-7610.00551 (2000).
- Grassi-Oliveira, R., Ashy, M. & Stein, L. M. Psychobiology of childhood maltreatment: effects of allostatic load? Revista Brasileira de Psiquiatria 30, 60-68, doi:10.1590/S1516-44462008000100012 (2008).
- McCrory, E., De Brito, S. A. & Viding, E. Research review: the neurobiology and genetics of maltreatment and adversity. Journal of Child Psychology and Psychiatry 51, 1079-1095, doi:10.1111/j.1469-7610.2010.02271.x (2010).
- McCrory, E., De Brito, S. A. & Viding, E. The impact of childhood maltreatment: a review of neurobiological and genetic factors. Frontiers in Psychiatry 2, 1-14, doi:10.3389/fpsyt.2011.00048 (2011).
- McCrory, E. J., Gerin, M. I. & Viding, E. Annual research review: childhood maltreatment, latent vulnerability and the shift to preventative psychiatry – the contribution of functional brain imaging. Journal of Child Psychology and Psychiatry 58, 338-357, doi:10.1111/jcpp.12713 (2017).
- Teicher, M. H. et al. The neurobiological consequences of early stress and childhood maltreatment. Neurosci. Biobehav. Rev. 27, 33-44, doi:10.1016/S0149-7634(03)00007-1 (2003).
- Twardosz, S. & Lutzker, J. R. Child maltreatment and the developing brain: a review of neuroscience perspectives. Aggression and Violent Behavior 15, 59-68, doi:10.1016/j.avb.2009.08.003 (2010).
- Heany, S. J. et al. The neural correlates of Childhood Trauma Questionnaire scores in adults: a meta-analysis and review of functional magnetic resonance imaging studies. Dev. Psychopathol. 30, 1475-1485, doi:10.1017/S0954579417001717 (2018).
- Hein, T. C. & Monk, C. S. Research review: neural response to threat in children, adolescents, and adults after child maltreatment – a quantitative meta-analysis. The Journal of Child Psychology and Psychiatry 58, 222-230, doi:10.1111/jcpp.12651 (2017).
- 68 Pechtel, P. & Pizzagalli, D. A. Effects of early life stress on cognitive and affective function: an integrated review of human literature. Psychopharmacology (Berl). 214, 55-70, doi:10.1007/s00213-010-2009-2 (2011).
- Herzberg, M. P. & Gunnar, M. R. Early life stress and brain function: activity and connectivity associated with processing emotion and reward. Neuroimage 209, 116493, doi:10.1016/j.neuroimage.2019.116493 (2020).
- McCrory, E. J., Ogle, J. R., Gerin, M. I. & Viding, E. Neurocognitive adaptation and mental health vulnerability following maltreatment: the role of social functioning. Child Maltreatment 24, 435-451, doi:10.1177/1077559519830524 (2019).
- Pollak, S. D. Multilevel developmental approaches to understanding the effects of child maltreatment: recent advances and future challenges. Dev. Psychopathol. 27, 1387-1397, doi:10.1017/S0954579415000826 (2015).
- Danese, A. et al. The origins of cognitive deficits in victimized children: implications for neuroscientists and clinicians. Am. J. Psychiatry 174, 349-361, doi:10.1176/appi.ajp.2016.16030333 (2017).
- Cicchetti, D. Annual research review: resilient functioning in maltreated children – past, present, and future perspectives. Journal of Child Psychology and Psychiatry 54, 402-422, doi:10.1111/j.1469-7610.2012.02608.x (2013).
- Cowell, R. A., Cicchetti, D., Rogosch, F. A. & Toth, S. L. Childhood maltreatment and its effect on neurocognitive functioning: timing and chronicity matter. Dev. Psychopathol. 27, 521-533, doi:10.1017/S0954579415000139 (2015).
- Bücker, J. et al. Cognitive impairment in school-aged children with early trauma. Compr. Psychiatry 53, 758-764, doi:10.1016/j.comppsych.2011.12.006 (2012).
- Beers, S. R. & De Bellis, M. D. Neuropsychological function in children with maltreatment-related posttraumatic stress disorder. Am. J. Psychiatry 159, 483-486, doi:10.1176/appi.ajp.159.3.483 (2002).
- De Bellis, M. D., Hooper, S. R., Spratt, E. G. & Woolley, D. P. Neuropsychological findings in childhood neglect and their relationships to pediatric PTSD. J. Int. Neuropsychol. Soc. 15, 868-878, doi:10.1017/S1355617709990464 (2009).
- DePrince, A. P., Weinzierl, K. M. & Combs, M. D. Executive function performance and trauma exposure in a community sample of children. Child Abuse Negl. 33, 353-361, doi:10.1016/j.chiabu.2008.08.002 (2009).
- Nolin, P. & Ethier, L. Using neuropsychological profiles to classify neglected children with or without physical abuse. Child Abuse Negl. 31, 631-643, doi:10.1016/j.chiabu.2006.12.009 (2007).
- 80 Mezzacappa, E., Kindlon, D. & Earls, F. Child abuse and performance task assessments of executive functions in boys. Journal of Child Psychology and Psychiatry 42, 1041-1048, doi:10.1111/1469-7610.00803 (2001).
- Vasilevski, V. & Tucker, A. Wide-ranging cognitive deficits in adolescents following early life maltreatment. Neuropsychology 30, 239-246, doi:10.1037/neu0000215 (2016).
- Gray, P., Baker, H. M., Scerif, G. & Lau, J. Y. F. Early maltreatment effects on adolescent attention to non-emotional and emotional distractors. Australian Journal of Psychology 68, 143-153, doi:10.1111/ajpy.12139 (2016).
- Mothes, L. et al. Childhood maltreatment and executive functions in adolescents. Child and Adolescent Mental Health 20, 56-62, doi:10.1111/camh.12068 (2015).
- Rogosch, F. A., Cicchetti, D. & Aber, J. L. The role of child maltreatment in early deviations in cognitive and affective processing abilities and later peer relationship problems. Dev. Psychopathol. 7, 591-609, doi:10.1017/S0954579400006738 (1995).
- Masson, M., Bussières, E.-L., East-Richard, C., R-Mercier, A. & Cellard, C. Neuropsychological profile of children, adolescents and adults experiencing maltreatment: a meta-analysis. The Clinical Neuropsychologist 29, 573-594, doi:10.1080/13854046.2015.1061057 (2015).
- Davis, A. S., Moss, L. E. & Nogin, M. M. Neuropsychology of child maltreatment and implications for school psychologists. Psychology in the Schools 52, 77-91, doi:10.1002/pits.21806 (2015).
- McLean, S. The effect of trauma on the brain development of children: evidence-based principles for supporting the recovery of children in care. (Child Family Community Australia, 2016).
- Irigaray, T. Q. et al. Child maltreatment and later cognitive functioning: a systematic review. Psicologia: Refl exão e Crítica 26, 376-387, doi:10.1590/S0102-79722013000200018 (2013).
- Eckenrode, J., Laird, M. & Doris, J. School performance and disciplinary problems among abused and neglected children. Dev. Psychol. 29, 53-62, doi:10.1037/0012-1649.29.1.53 (1993).
- Jenness, J. L. et al. Violence exposure and neural systems underlying working memory for emotional stimuli in youth. Dev. Psychopathol. 30, 1517-1528, doi:10.1017/S0954579417001638 (2018).
- Bolger, K. E., Patterson, C. J. & Kupersmidt, J. B. Peer relationships and self-esteem among children who have been maltreated. Child Dev. 69, 1171-1197, doi:10.1111/j.1467-8624.1998.tb06166.x (1998).
- Bolger, K. E. & Patterson, C. J. Developmental pathways from child maltreatment to peer rejection. Child Dev. 72, 549–568, doi:10.1111/1467-8624.00296 (2001).
- Carrion, V. G., Garrett, A., Menon, V., Weems, C. F. & Reiss, A. L. Posttraumatic stress symptoms and brain function during a response-inhibition task: an fMRI study in youth. Depress. Anxiety 25, 514-526, doi:10.1002/da.20346 (2008).
- Mueller, S. C. et al. Early-life stress is associated with impairment in cognitive control in adolescence: an fMRI study. Neuropsychologia 48, 3037-3044, doi:10.1016/j.neuropsychologia.2010.06.013 (2010).
- Bruce, J. et al. Patterns of brain activation in foster children and nonmaltreated children during an inhibitory control task. Dev. Psychopathol. 25, 931-941, doi:10.1017/S095457941300028X (2013).
- Jankowski, K. F. et al. Preliminary evidence of the impact of early childhood maltreatment and a preventative intervention on neural patterns of response inhibition in early adolescence. Developmental Science 20, 1-15, doi:10.1111/desc.12413 (2016).
- Hart, H. et al. Reduced functional connectivity of fronto-parietal sustained attention networks in severe childhood abuse. PLoS One 12, e0188744, doi:10.1371/journal.pone.0188744 (2017).
- Lim, L. et al. Neurofunctional abnormalities during sustained attention in severe childhood abuse. PLoS One 11, e0165547, doi:10.1371/journal.pone.0165547 (2016).
- Hart, H. et al. Altered functional connectivity of fronto-cingulo-striatal circuits during error monitoring in adolescents with a history of childhood abuse. Frontiers in Human Neuroscience 12, 1-15, doi:10.3389/fnhum.2018.00007 (2018).
- Lim, L. et al. Neural correlates of error processing in young people with a history of severe childhood abuse: an fMRI study. Am. J. Psychiatry 172, 892-900, doi:10.1176/appi.ajp.2015.14081042 (2015).
- Gerin, M. I. et al. A neurocomputational investigation of reinforcement-based decision making as a candidate latent vulnerability mechanism in maltreated children. Dev. Psychopathol. 29, 1689-1705, doi:10.1017/S095457941700133X (2017).
- Meyer, A. M. et al. Self-reported and observed punitive parenting prospectively predicts increased error-related brain activity in six-year-old children. J. Abnorm. Child Psychol. 43, 821-829, doi:10.1007/s10802-014-9918-1 (2015).
- Guyer, A. E. et al. Behavioral alterations in reward system function: the role of childhood maltreatment and psychopathology. J. Am. Acad. Child Adolesc. Psychiatry 45, 1059-1067, doi:10.1097/01.chi.0000227882.50404.11 (2006).
- Kasparek, S. W., Jenness, J. L. & McLaughlin, K. A. Reward processing modulates the association between trauma exposure and externalizing psychopathology. Clinical Psychological Science 8, 989-1006, doi:10.1177/2167702620933570 (2020).
- Hanson, J. L. et al. Early adversity and learning: implications for typical and atypical behavioral development. Journal of Child Psychology and Psychiatry 58, 770-778, doi:10.1111/jcpp.12694 (2017).
- Hanson, J. L., Hariri, A. R. & Williamson, D. E. Blunted ventral striatum development in adolescence reflects emotional neglect and predicts depressive symptoms. Biol. Psychiatry 78, 598-605, doi:10.1016/j.biopsych.2015.05.010 (2015).
- Harms, M. B., Bowen, K. E. S., Hanson, J. L. & Pollak, S. D. Instrumental learning and cognitive flexibility processes are impaired in children exposed to early life stress. Developmental Science 21, e12596, doi:10.1111/desc.12596 (2018).
- da Silva Ferreira, G. C., Crippa, J. A. S. & de Lima Osório, F. Facial emotion processing and recognition among maltreated children: a systematic literature review. Frontiers in Psychology 5, 1-10, doi:10.3389/fpsyg.2014.01460 (2014).
- Luke, N. & Banerjee, R. Differentiated associations between childhood maltreatment experiences and social understanding: a meta-analysis and systematic review. Dev. Rev. 33, 1-28, doi:10.1016/j.dr.2012.10.001 (2013).
- During, S. M. & McMahon, R. J. Recognition of emotional facial expressions by abusive mothers and their children. J. Clin. Child Psychol. 20, 132-139, doi:10.1207/s15374424jccp2002_4 (1991).
- Pears, K. C. & Fisher, P. A. Emotion understanding and theory of mind among maltreated children in foster care: evidence of deficits. Dev. Psychopathol. 17, 47-65, doi:10.10170S0954579405050030 (2005).
- Pollak, S. D., Cicchetti, D., Hornung, K. & Reed, A. Recognizing emotion in faces: developmental effects of child abuse and neglect. Dev. Psychol. 36, 679-688, doi:10.1037//0012-1649.36.5.679 (2000).
- Sullivan, M. W., Bennett, D. S., Carpenter, K. & Lewis, M. Emotion knowledge in young neglected children. Child Maltreatment 13, 301-306, doi:10.1177/1077559507313725 (2008).
- Pollak, S. D. & Sinha, P. Effects of early experience on children’s recognition of facial displays of emotion. Dev. Psychol. 38, 784-791, doi:10.1037//0012-1649.38.5.784 (2002).
- Pollak, S. D. & Tolley-Schell, S. A. Selective attention to facial emotion in physically abused children. J. Abnorm. Psychol. 112, 323-338, doi:10.1037/0021-843X.112.3.323 (2003).
- Masten, C. L. et al. Recognition of facial emotions among maltreated children with high rates of post-traumatic stress disorder. Child Abuse Negl. 32, 139-153, doi:10.1016/j.chiabu.2007.09.006 (2008).
- Pollak, S. D., Messner, M., Kistler, D. J. & Cohn, J. F. Development of perceptual expertise in emotion recognition. Cognition 110, 242-247, doi:10.1016/j.cognition.2008.10.010 (2009).
- Curtis, W. J. & Cicchetti, D. Affective facial expression processing in 15 month-old infants who have experienced maltreatment: an event-related potential study. Child Maltreatment 18, 140-154, doi:10.1177/1077559513487944 (2013).
- Cicchetti, D. & Curtis, W. J. An event-related potential study of the processing of affective facial expressions in young children who experiences maltreatment during the first year of life. Dev. Psychopathol. 17, 641-677, doi:10.10170S0954579405050315 (2005).
- Pollak, S. D., Cicchetti, D., Klorman, R. & Brumaghim, J. T. Cognitive brain event-related potentials and emotion processing in maltreated children. Child Dev. 68, 773-787, doi:10.2307/1132032 (1997).
- Pollak, S. D., Klorman, R., Thatcher, J. E. & Cicchetti, D. P3b reflects maltreated children’s reactions to facial displays of emotion. Psychophysiology 38, 267-274, doi:10.1111/1469-8986.3820267 (2001).
- Pollak, S. D. Mechanisms linking early experience and the emergence of emotions: illustrations from the study of maltreated children. Current Directions in Psychological Science 17, 370-375, doi:10.1111/j.1467-8721.2008.00608.x (2008).
- Shackman, J. E., Shackman, A. J. & Pollak, S. D. Physical abuse amplifies attention to threat and increases anxiety in children. Emotion 7, 838-852, doi:10.1037/1528-3542.7.4.838 (2007).
- Shackman, J. E. & Pollak, S. D. Impact of physical maltreatment on the regulation of negative affect and aggression. Developmental Psychopathology 26, 1021-1033, doi:10.1017/S0954579414000546 (2014).
- Shields, A. & Cicchetti, D. Reactive aggression among maltreated children: the contributions of attention and emotion dysregulation. J. Clin. Child Psychol. 27, 381-395, doi:10.1207/s15374424jccp2704_2 (1998).
- Hart, H. et al. Altered fear processing in adolescents with a history of severe childhood maltreatment: an fMRI study. Psychol. Med. 48, 1092-1101, doi:10.1017/S0033291716003585 (2018).
- Maheu, F. S. et al. A preliminary study of medial temporal lobe function in youths with a history of caregiver deprivation and emotional neglect. Cognitive, Affective, & Behavioral Neuroscience 10, 34-49, doi:10.3758/CABN.10.1.34 (2010).
- Blair, K. S. et al. Sexual abuse in adolescents is associated with atypically increased responsiveness within regions implicated in self-referential and emotional processing to approaching animate threats. Frontiers in Psychiatry 11, 1-9, doi:10.3389/fpsyt.2020.00345 (2020).
- Bogdan, R., Williamson, D. E. & Hariri, A. R. Mineralocorticoid receptor iso/val (rs5522) genotype moderates the association between previous childhood emotional neglect and amygdala reactivity. Am. J. Psychiatry 169, 515-522, doi:10.1176/appi.ajp.2011.11060855 (2012).
- McCrory, E. J. et al. Amygdala activation in maltreated children during pre-attentive emotional processing. The British Journal of Psychiatry 202, 269-276, doi:10.1192/bjp.bp.112.116624 (2013).
- Garrett, A. S. et al. Brain activation to facial expressions in youth with PTSD symptoms. Depress. Anxiety 29, 449-459, doi:10.1002/da.21892 (2012).
- White, M. G. et al. FKBP5 and emotional neglect interact to predict individual differences in amygdala reactivity. Genes, Brain and Behavior 11, 869-878, doi:10.1111/j.1601-183X.2012.00837.x (2012).
- McLaughlin, K. A., Peverill, M., Gold, A. L., Alves, S. & Sheridan, M. A. Child maltreatment and neural systems underlying emotion regulation. J. Am. Acad. Child Adolesc. Psychiatry 54, 753-762, doi:10.1016/j.jaac.2015.06.010 (2015).
- Jenness, J. L. et al. Alterations in neural circuits underlying emotion regulation following child maltreatment: a mechanism underlying trauma-related psychopathology. Psychol. Med., 1-10, doi:10.1017/S0033291720000641 (in press).
- Marusak, H. A., Martin, K. R., Etkin, A. & Thomason, M. E. Childhood trauma exposure disrupts the automatic regulation of emotional processing. Neuropsychopharmacology 40, 1250-1258, doi:10.1038/npp.2014.311 (2015).
- Wymbs, N. F. et al. Social supports moderate the effects of child adversity on neural correlates of threat processing. Child Abuse Negl. 102, 104413, doi:10.1016/j.chiabu.2020.104413 (2020).
- Raby, K. L. et al. The legacy of early abuse and neglect for social and academic competence from childhood to adulthood. Child Dev. 90, 1684-1701, doi:10.1111/cdev.13033 (2019).
- Matheson, S. L. et al. Effects of maltreatment and parental schizophrenia spectrum disorders on early childhood social-emotional functioning: a population record linkage study. Epidemiology and Psychiatric Sciences 26, 612-623, doi:10.1017/S204579601600055X (2017).
- Australian Centre for Posttraumatic Mental Health & Parenting Research Centre. Approaches targeting outcomes for children exposed to trauma arising from abuse and neglect: evidence, practice and implications. Report prepared for the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs. (The Australian Center for Posttraumatic Mental Health, Carlton, Victoria, 2014).
- Dorsey, S. et al. Evidence base update for psychosocial treatments for children and adolescents exposed to traumatic events. Journal of Clinical Child & Adolescent Psychology 46, 303-330, doi:10.1080/15374416.2016.1220309 (2017).
- Fraser, J. G. et al. A comparative effectiveness review of parenting and trauma-focused interventions for children exposed to maltreatment. J. Dev. Behav. Pediatr. 34, 355-368, doi:10.1097/DBP.0b013e31828a7dfc (2013).
- Macdonald, G. et al. The effectiveness, acceptability and cost-effectiveness of psychosocial interventions for maltreated children and adolescents: an evidence synthesis. Health Technol. Assess. 20, doi:10.3310/hta20690 (2016).
- Navalta, C. P., McGee, L. & Underwood, J. Adverse childhood experiences, brain development, and mental health: a call for neurocounseling. Journal of Mental Health Counseling 40, 266-278, doi:10.17744/mehc.40.3.07 (2018).
- Jaffee, S. R. & Christian, C. W. The biological embedding of child abuse and neglect: implications for policy and practice. Social Policy Report 28, 3-19, doi:10.1002/j.2379-3988.2014.tb00078.x (2014).
- Fung, A. & Ricci, M. F. Rethinking ‘essential’ and ‘nonessential’: the developmental paediatrician’s COVID-19 response. Paediatrics & Child Health 25, 265-267, doi:10.1093/pch/pxaa077 (2020).
- Ramtekkar, U. et al. Pediatric telebehavioral health: a transformational shift in care delivery in the era of COVID-19. JMIR Mental Health 7, e20157, doi:10.2196/20157 (2020).
- Racine, N., Hartwick, C., Collin-Vézina, D. & Madigan, S. Telemental health for child trauma treatment during and post-COVID-19: limitations and considerations. Child Abuse Negl., doi:10.1016/j.chiabu.2020.104698 (in press).
- Fazel, M., Patel, V., Thomas, S. & Tol, W. Mental health interventions in schools in low-income and middle-income countries. Lancet Psychiatry 1, 388-398, doi:10.1016/S2215-0366(14)70357-8 (2014).
- Fazel, M., Hoagwood, K., Stephan, S. & Ford, T. Mental health interventions in schools in high-income countries. Lancet Psychiatry 1, 377-387, doi:10.1016/S2215-0366(14)70312-8 (2014).
- M’jid, N. M. Hidden scars: the impact of violence and the COVID-19 pandemic on children’s mental health. Child and Adolescent Psychiatry and Mental Health 14, 1-3, doi:10.1186/s13034-020-00340-8 (2020).
- Centers for Disease Control and Prevention. Preventing child maltreatment through the promotion of safe, stable, and nurturing relationships between children and caregivers. (CDC, Atlanta, GA).
- World Health Organization (WHO). Preventing violence through the development of safe, stable and nurturing relationships between children and their parents and caregivers. (Geneva, Switzerland, 2009).
- Fortson, B. L., Klevins, J., Merrick, M. T., Gilbert, L. K. & Alexander, S. P. Preventing child abuse and neglect: a technical package for policy, norm, and programmatic activities. (Division of Violence Prevention, National Center for Injury Prevention and Control, Center for Disease Control and Prevention, Atlanta, Georgia, 2016).
- Camilo, C., Vaz Garrido, M. V. & Calheiros, M. M. The social information processing model in child physical abuse and neglect: a meta-analytic review. Child Abuse Negl. 108, 104666, doi:10.1016/j.chiabu.2020.104666 (2020).
- Toth, S. L., Gravener-Davis, J. A., Guild, D. J. & Cicchetti, D. Relational interventions for child maltreatment: past, present, and future perspectives. Dev. Psychopathol. 25, 1601-1617, doi:10.1017/S0954579413000795 (2013).
- Howe, T. R. et al. International child abuse prevention: insights from ACT Raising Safe Kids. Child and Adolescent Mental Health 22, 194-200, doi:10.1111/camh.12238 (2017).
- Knerr, W., Gardner, F. & Cluver, L. Improving positive parenting skills and reducing harsh and abusive parenting in low- and middle-income countries: a systematic review. Prevention Science 14, 352-363, doi:10.1007/s11121-012-0314-1 (2013).
- MacMillan, H. L. et al. Interventions to prevent child maltreatment and associated impairment. Lancet 373, 250-266, doi:10.1016/S0140-6736(08)61708-0 (2009).
- Wessels, I. et al. Preventing violence: evaluating outcomes of parenting programmes. (World Health Organization, Geneva, Switzerland, 2013).
- Mikton, C. et al. The assessment of the readiness of five countries to implement child maltreatment prevention programs on a large scale. Child Abuse Negl. 37, 1237-1251, doi:10.1016/j.chiabu.2013.07.009 (2013).
- UNICEF. Preventing and responding to violence against children and adolescents: theory of change. (United Nations Children’s Fund, New York, NY, 2017).
Appendix: A note on treatment
Because brains are modifiable (neuroplasticity) and can be changed through interactions with the environment, some of the effects of a negative environment can be counteracted by provision of a positive environment. Although not the focus of this brief, it is important to acknowledge treatment approaches for children, caregivers, and nations in the context of child maltreatment. In Article 19, the UN Convention on the Rights of the Child calls for protective measures including “the establishment of social programmes to provide necessary support for the child and for those who have the care of the child, as well as for other forms of prevention and… treatment and follow-up of instances of child maltreatment” 1.
In addressing the mental health symptoms of maltreatment in children, it is important to use evidence-based approaches so as not to waste time and resources on approaches that do not work; however, some practitioners may not be aware of or use evidence-based approaches 139. The post-traumatic stress, depressive, and anxiety symptoms that can occur in children who have been maltreated are treatable with therapy. In reviews, the efficacy of Cognitive Behavioral Therapy is well-established e.g., 139,140,141,142. Any therapy should acknowledge the complex biological, psychological, social, and cultural contexts of development e.g., 143, with a focus expanded beyond welfare to well-being e.g., 144, and should only be provided with assent of the child.
Pediatric telemedicine may be a viable option for such care 145,146. However, access to technology, lack of confidential space, and reluctance to process trauma in the absence of a safe environment may be challenges to telemedicine from home 147. Mental health interventions in schools may be even more crucial. But more evidence is needed regarding how effective interventions can be scaled up and implemented in schools in low- and middle-income countries 148. Integration of evidence-based mental health services within schools can democratize access 149. Unfortunately, globally, there “has been a lack of investment and capacity to provide quality, rights-based, culturally appropriate mental health care” 150, p. 1.
Whereas treating children is key, providing additional support to reduce stress and build coping and parenting strategies in caregivers is also important, especially in terms of advancing understanding of child development and building safe, stable, and nurturing relationships between caregivers and children e.g., 141,151,152-155. Evidence-based parenting interventions can both decrease harsh and increase nurturing parenting practices e.g., 156,157,158. Along with enhancing parenting skills and changing social norms to support positive parenting, strengthening economic support to families, providing quality early care and education, and early intervention are best-evidence strategies to help prevent child maltreatment e.g., 153.
There is evidence that affordable, flexible, evidence-informed programs for parents and children can be adapted and implemented in diverse cultural and economic contexts around the world e.g., 156,157,159. However, it is important to pre-determine the readiness of countries to implement evidence-based child maltreatment prevention programs on a large scale to increase the likelihood of success 160. At the national policy level, the World Health Organization has summarized seven research-based strategies to address all violence against children 36 and UNICEF has similarly advanced a detailed theory of change to guide work on preventing and responding to all violence against children, including pathways of change and a set of evidence-based strategies 161.